– Written by Venkatesan Balu, Associate Director, Global Data Sciences, Navitas Life Sciences
Amid the excitement over advancements in technology, I would like to shed light, as a statistician, on the role of biostatisticians in the emerging field of risk-based monitoring. Despite the release of the addendum to ICH-GCP-E6 in 2016, which emphasised the importance of risk-based and centralised monitoring, the implementation of these strategies has been slow. This can be attributed to the reluctance of sites and conventional monitoring services provided by CROs to move to the new changes. However, the pandemic has brought about a transformative period for all clinical research sites, forcing them to adapt and learn. This period has highlighted the need to enhance the adoption of technology while ensuring patient continuity and safety in offsite monitoring.
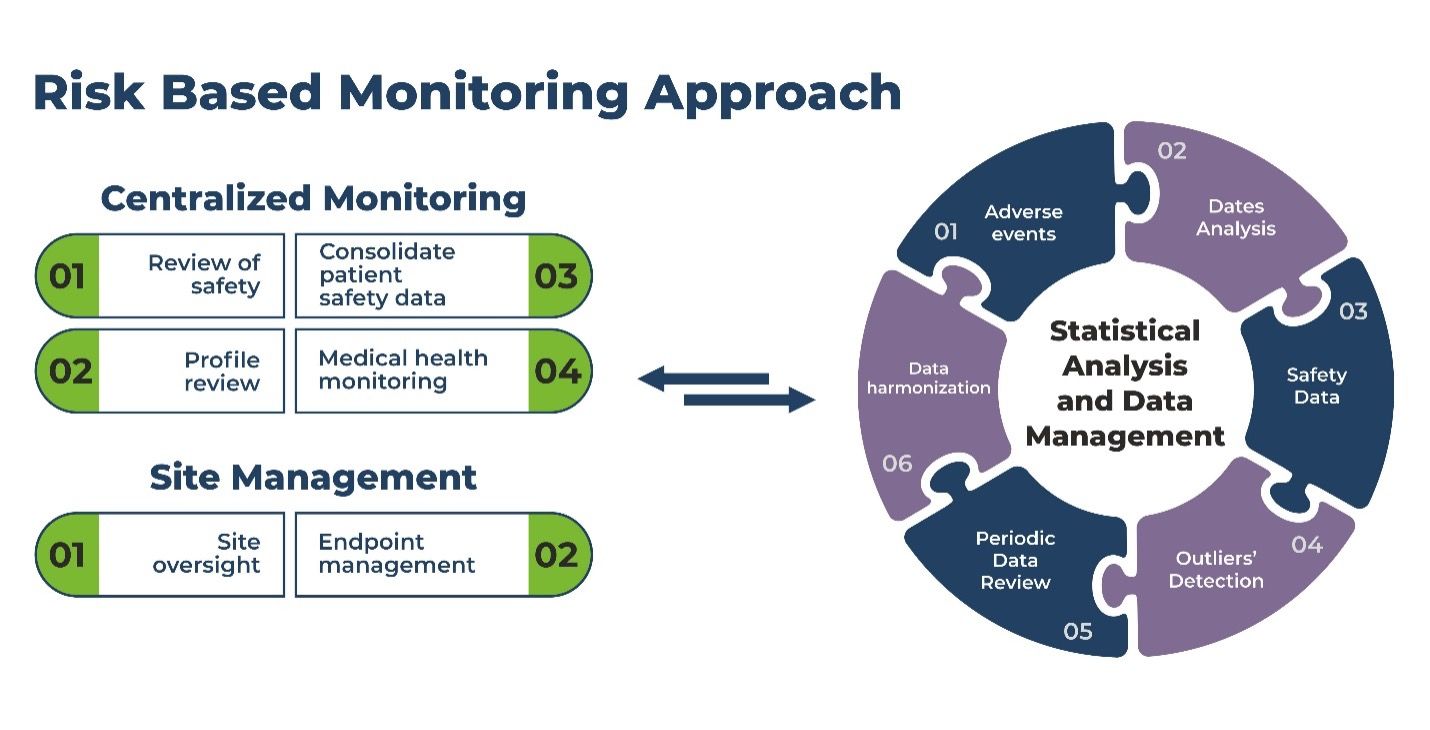
The increased frequency of offsite monitoring in clinical sites has resulted in a growing demand for the implementation of risk-based monitoring (RBM) and centralised monitoring (CM). In order to establish a strong centralised monitoring team, it is essential to include biostatisticians and statistical programmers who may not have been traditionally involved in onsite monitoring but play crucial roles in ensuring robust monitoring processes.
Risk-Based Monitoring (Onsite Monitoring) and Centralised Monitoring
Traditional onsite monitoring (TM), designed to identify risk and data errors, is built into protocols to occur periodically based on the needs of protocol and can be triggered by events requiring further investigation (e.g. screen failure). Advancements in technology has ensured significant strides in data management practices by enabling electronic data collection (such as eCRFs, tablets and wearables), making RBM and CM strategies easier to implement and improving TM efficiency. Examining data centrally and in real time, through computer analysis or formal statistical tests, enables identification of potential risks, which individuals might not spot. Problems can then be addressed proactively, reducing time and cost, and increasing the overall efficiency.
The RBM and CM team, or the medical monitor, should work with the TM team to facilitate better execution. They should identify when TM is required, at which sites or regions, and to what degree; for example, whether a phone call or an in-person visit is required.
The Need for Statisticians and Programmers
Let us understand the need for biostatisticians and statistical programmers. Though the collected data remains the same, statistical expertise in generating accurate descriptions of trial data and to interpret and analyses appropriately is needed.
The main objective of statistical risk-based monitoring is to precisely identify the potential risks that could arise from specific sites or investigators, staff who may require additional training, geographic location of the sites, sponsor interventions and error in recording or fraud. Moreover, statistical risk-based monitoring not only enhances the quality of data but also reduces the overall cost of the study by reducing the number of onsite visits.
Here are some exciting methods or examples used to identify potential risk in the data using techniques like supplementary statistical analysis, data pattern identification, pictorial/graphical analysis, and anomalous/outlier detection.
How Statistical Interpretations for Risk Help Improve Efficiencies
**Adverse Events:**AE data is the most important safety data to be considered and interpreted in clinical data. Statistical analysis to compare the proportion of subjects with AEs by site could enable operational teams to identify any discrepancies and investigate the quality of reporting. This proactive approach reduces the likelihood of unnoticed events and ensures proper notification.
**Dates:**Programmatic analysis of dates will help identify potential issues such as missing records, identical records, subjects attending on unexpected dates and the appearance of subjects.
Safety Parameters: Analysing trends in safety parameters provides clearer insights into the data. Statistical analysis like analysis of variance (ANOVA) and mixed models for repeated measures (MMRM) can be used to investigate differences and/or similarities across sites for lab parameters or sets of lab parameters. However, statistical cognisance is required when interpreting the results of these analyses due to multiplicity.
**Outlier Detections:**All the anomalous safety parameters for patients which are either considerably lower or higher from the mean can be detected using centralised monitoring. For non-normal data, the interquartile range (IQR) can be used to identify patients with values lying outside a specified range. These patients can then be investigated further to assess the nature and significance of their data deviations.
Univariate analyses examine each parameter separately through data visualisations such as box plots and by identifying outlying patients for each parameter using Grubbs’ method or similar. On the other hand, multivariate analyses consider a set of parameters by using Mahalanobis distance, which measures the distance of each patient’s parameter set from the average, taking into account the correlation between the variables. These distances can help identify both outliers and inliers when the negative logarithm is applied. Patients and sites exhibiting extreme values can be flagged and investigated further by the clinical team to gain insights and take appropriate actions based on the results.
Using Statistical Analysis Responsibly
The detection and identification of risks in the data are vital for supporting the clinical team during routine monitoring visits. However, the quality of risk identification can be significantly enhanced through the implementation of statistical risk-based monitoring (SRBM). By employing systematic and consistent analyses, along with statistically validated programs, SRBM enables the processing of large amounts of data to assess risk more effectively. Statisticians play a critical role in performing these analyses and providing their expertise in interpreting the extensive data involved in clinical trials. They not only develop the necessary programs but also devise techniques and interpret results and trends to inform clinical monitoring teams about potential risks and errors. As SRBM and CM continue to evolve, different methods may be required for each trial, underscoring the ongoing need for statisticians and programmers as integral members of the SRBM and CM teams, ensuring robust risk assessment and comprehensive SRBM and/or CM implementation.

Venkatesan Balu is Associate Director, Global Data Sciences, Navitas Life Sciences, with 15+ years of experience in the biostatistics domain, and in Phase I to Phase IV clinical trials across various therapeutic areas, BABE and PK studies. He has invaluable expertise in providing inputs to study design, sample size, SAP, outlier evaluation, interim analysis, complex statistical evaluation and model selection, and regulatory requirements. Venkatesan is a technical leader in drug development strategy, adaptive design, portfolio optimisation, and decision-making in clinical trials.